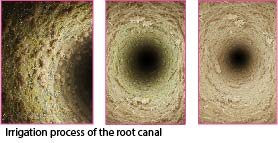
How do endodontists perform irrigation in Post-Endodontic reconstruction?
How do we kill bacteria and dissolve organic tissue ? 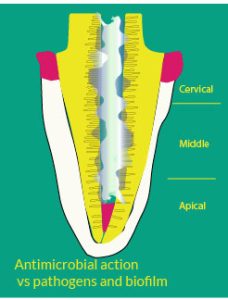
Endodontists must engage an organic battle, kill bacteria (All of them!) and dissolve the pulp tissue.
In doing so, one must be gentle with the dentinal wall and grant the dentinal structure to facilitate the formation of tags during the subsequent Post-Endodontic reconstruction. That means: open the tubules properly without destroying the root canal overall structure, especially the peritubular dentin.
1 – The champion, by many, is considered the Sodium Hypochlorite (NaOCl). A reducing agent. Its concentration might vary upon the clinician’s preferences. A 5.25% is widely used by the majority of the endodontists. However, many others prefer a lower concentration (ranging from 0.5 to 5%), in a trade-off between less antimicrobial efficiency and more “safety” related to the dentin demineralization and level of toxicity. Others push the %age of chlorine concentration up to 6%, and even slightly more to increase the antimicrobial efficiency.
2 – An antiseptic doing this job well is also the Chlorhexidine (CHX). 2 Characteristics: antimicrobial effect and inhibitory action on MMPs; zinc-dependent enzymes that degrade components of the extracellular matrix, such as collagen.
Therefore, which one works better?
The answer is not straightforward.
What do we ask to the above irrigants? Simply, to kill bacteria and dissolve the pulp tissue. 
Don’t forget that other actors will participate at the irrigation process (think about the inorganic battle). A vast majority of practitioners and academics agree that Sodium Hypochlorite ( NaOCl) does an excellent job in both respects! We dare to say. The best job.
Chlorhexidine (CHX) is also a viable and respectable option for its broad antimicrobial spectrum. A 2% concentration is very effective, for instance, against E. Faecalis.
But is CHX as effective as NaOCl to dissolve pulp tissue and efficiently dissolve the biofilm? Furthermore, does it promote a long-term dentin bonding to resins thanks to its substantivity (remains in dentine)?
The debate is open. What irrigant shall one pick up from the shelf?
By listening to and reading a vast number of opinions and academics, we can draft some conclusions.
Both NaOCl and CHX are aimed at removing the smear layer, exposing collagen fibers, and decontaminating the root surface to enhance the success of adhesion techniques.
Both of them grant a good level of antimicrobial efficacy, low level of cytotoxicity, and high substantivity, with NaOCl having a more effective chelating action and CHX proposing a trade-off with its anti MMPs action.
It seems there isn’t a clear winner. The preference is mostly left to the tradition of practice and individual preferences of the doctors.
Is there a third, fourth, fifth alternative to the above products?
Traditionally, products that can play the organic battle are:
- Hydrogen Peroxide (H2O2), which brings about a good level of effervescence and bubbling ( fundamental in smear layer removal).
- MTAD– Mixture of Tetracycline, Acid (Citric), and Detergent- Also used as an antimicrobial with a multitasking action. Often it is used for the final rinse, sometimes, after NaOCl, to remove the smear layer.
In conclusion, if we look at statistics and literature, it appears that NaOCl is preferred by many, strictly, in relation to the efficiency in terms of antimicrobial effect and necrotic and pulp tissue dissolving. Therefore, it is the “elected” first product. On the other hand, CHX also delivers an efficient job in these terms. In addition, a vast majority of Endodontists prefer to use the CHX after the acid etchant and before the adhesive, to inhibit MMPs and stabilize the adhesive interface.
It looks that both, these 2 products, must be within reach of every dentist.